What Is a 4-Panel Drug Test? A Complete 2026 Employer Guide
A 4-panel drug test is a urine-based, point-of-collection (POC) immunoassay screen that detects four classes of drugs — most commonly built by removing one substance (typically THC) from the standard SAMHSA 5-panel — used by non-DOT-regulated employers who want a quick, affordable, defensible workplace drug-screening program. It is a screening tool only; any non-negative result must be confirmed by a SAMHSA-certified laboratory and reviewed by a Medical Review Officer (MRO) before any employment action.
The 4-panel drug test is one of the most widely used workplace drug-screening configurations in the United States — but it’s also one of the most misunderstood. Employers conflate it with the federal 5-panel; result interpretation gets read backwards more often than you’d think; and the regulatory landscape around drug testing changed substantially in 2023–2025 with the addition of oral fluid testing, fentanyl, and the latest SAMHSA Mandatory Guidelines.
This guide is the 2026 update — written for HR, safety, and compliance leaders who need a defensible drug-testing program that holds up to MRO review and legal scrutiny.
Key Takeaways
What it is: A urine immunoassay screen that detects four drug classes. Unlike the federal 5-panel (governed by SAMHSA Mandatory Guidelines), there is no single national standard for what the four classes contain — composition is set by the employer or testing provider.
Most common configuration today: The “no-THC” variant — amphetamines, cocaine, opiates, and PCP — used by employers in states with legalized recreational marijuana who still want a drug-free workplace policy.
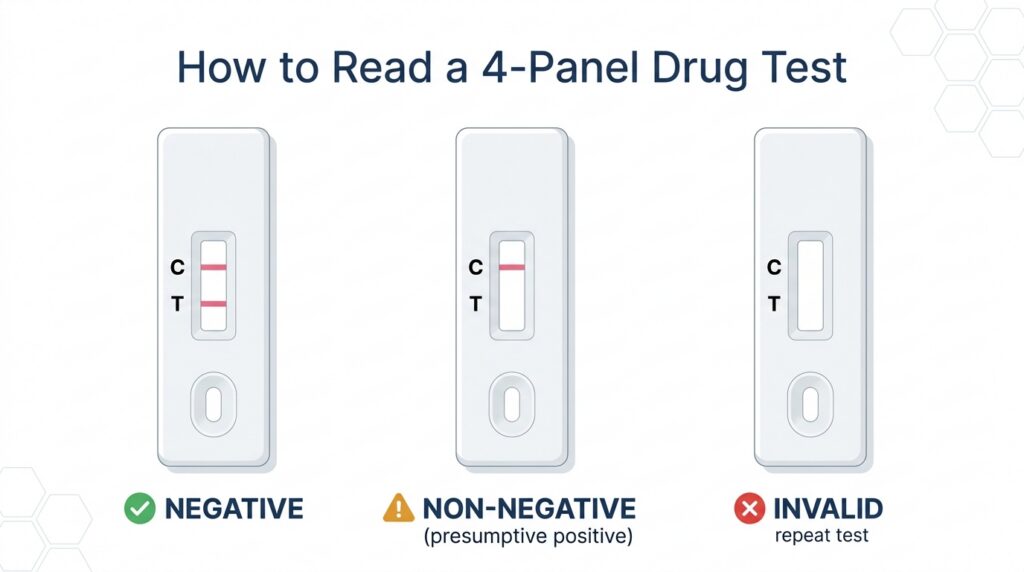
Reading results — the critical rule: Any visible line in the Test (T) region — even a faint one — is NEGATIVE. No line in the T region (with a Control (C) line present) is a Non-Negative / presumptive positive. (The original version of this article had this reversed — corrected in this 2026 update.)
Always lab-confirmed. A POC screen never decides employment outcomes alone. Non-negative results are sent to a SAMHSA-certified laboratory for GC-MS or LC-MS/MS confirmation, then reviewed by a Medical Review Officer (MRO) before reporting to the employer.
Sample requirements: ~30–45 mL urine; temperature must read 90–100°F within 4 minutes of collection.
Detection windows: Roughly 2–3 days for cocaine/methamphetamine; 1–7+ days for marijuana (occasional vs. chronic use); 1–3 days for most opiates.
Not for DOT-regulated employees. Federally regulated transportation, aviation, rail, pipeline, and maritime workers must follow the DOT 5-panel under 49 CFR Part 40, which now also includes fentanyl (added by HHS to federal panels effective July 7, 2025; DOT harmonization in progress).
Use case fit: Pre-employment screening, random testing, post-incident testing, reasonable suspicion testing, return-to-duty / follow-up testing — for non-DOT workforces.
Table of Contents
What is a 4 Panel Drug Test
A 4-panel drug test is a urine-based screening test that uses competitive-binding immunoassay technology to detect the presence of four specific drug classes — or four specific drugs — at or above predetermined cutoff levels.
Crucially, unlike the DOT 5-panel (mandated by 49 CFR Part 40) or the SAMHSA federal workplace 5-panel (governed by the HHS Mandatory Guidelines), there is no universal standard for which four substances appear in a 4-panel test. The composition is set by the employer or third-party administrator, typically by:
Removing one substance from the standard SAMHSA 5-panel (most commonly THC), or
Building a custom panel of four substances based on industry risk, local drug-use trends, and state law.
Most 4-panel tests are administered as point-of-collection (POC) rapid screens — dip cards, cassettes, or integrated cups — that produce a visual screening result in about 5 minutes. They are screening tools, not diagnostic tools: every non-negative result requires laboratory confirmation and MRO review before any employment decision.
What Substances Does a 4-Panel Drug Test Detect?
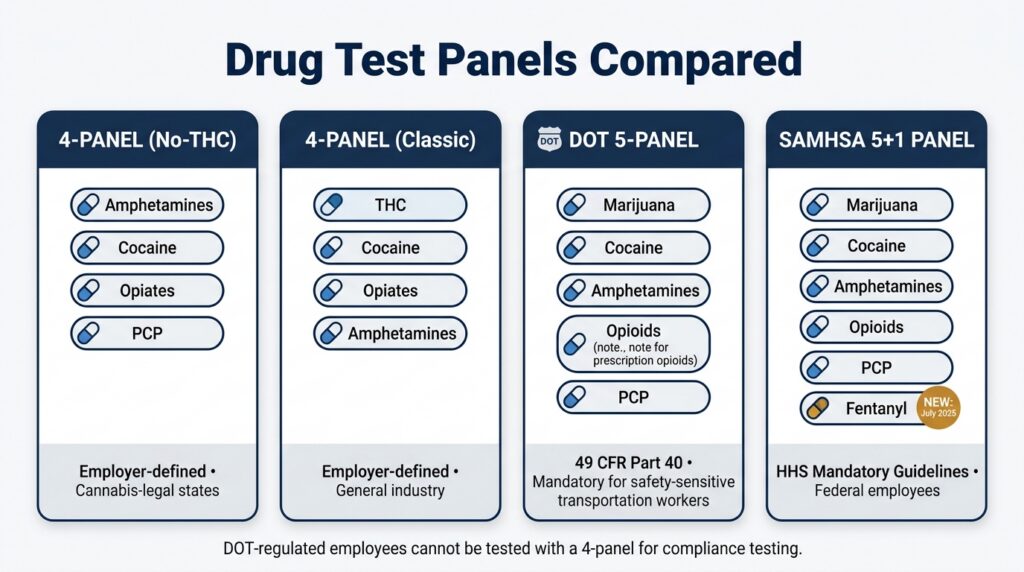
The two most common 4-panel configurations in 2026:
Configuration A — “No-THC” (most common today)
For employers in states with legalized recreational marijuana who want a drug-free workplace without testing for THC:
Amphetamines (including methamphetamine and MDMA in some panels)
Cocaine
Opiates (codeine, morphine, heroin metabolites)
PCP (phencyclidine)
Configuration B — Classic four (common in older / general industry)
The configuration originally described in this article:
Marijuana / THC
Cocaine
Opiates
Amphetamines / Methamphetamines
What’s not in a standard 4-panel
Important to flag for employers, because misunderstanding here drives most workplace drug-testing complaints:
Fentanyl — not in standard 4-panel tests; requires explicit add-on. (Now in SAMHSA federal workplace panels effective July 7, 2025; DOT harmonization rule proposed Sept 2, 2025.)
Benzodiazepines (Xanax, Valium, Ativan), methadone, oxycodone/oxymorphone/hydrocodone/hydromorphone, buprenorphine, tramadol, synthetic opioids generally — not detected by standard opiate immunoassay; require expanded or custom panels.
Alcohol — never part of a urine drug panel; tested separately via breath alcohol or EtG/EtS urine testing.
Practical implication: If your workforce risk profile includes prescription-opioid misuse, fentanyl exposure, or benzodiazepine diversion, a standard 4-panel will systematically miss those — you likely need a 9-, 10-, or 12-panel test, or a custom configuration.
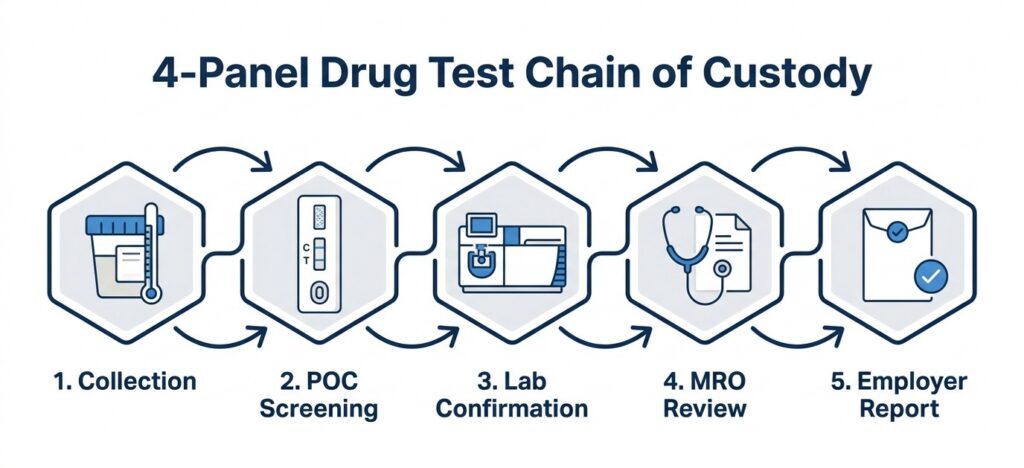
How a 4-Panel Drug Test Works (Step-by-Step)
A defensible POC 4-panel collection follows a tightly choreographed protocol — derived from the SAMHSA Specimen Collection Handbook even when the test itself isn’t federally regulated:
Privacy and integrity controls — bluing agent in toilet bowl, water source secured, soap removed.
Specimen collection — donor provides a urine specimen of at least 30–45 mL (45 mL is the federal standard) into a sealed, single-use collection container.
Temperature check within 4 minutes — temperature strip on the cup must read between 90–100°F (32–38°C). Out-of-range readings indicate possible adulteration or substitution.
Specimen integrity validation — many cups also include adulterant strips (pH, specific gravity, creatinine, oxidants) to detect dilution or tampering.
Initial screen — the test cassette or integrated cup strips are exposed to the urine. Results develop over 3–8 minutes depending on the device.
Read results within the manufacturer’s window — typically at the 5-minute mark; do not interpret after the upper time limit (often 8–10 minutes).
For any non-negative screening result — the specimen is sealed, chain-of-custody documentation completed, and shipped to a SAMHSA-certified laboratory for confirmatory testing using gas chromatography–mass spectrometry (GC-MS) or liquid chromatography–tandem mass spectrometry (LC-MS/MS).
MRO review — the laboratory’s confirmed result is reviewed by a Medical Review Officer (MRO), a licensed physician trained and certified in substance abuse testing, who interviews the donor about prescription medications and other legitimate medical explanations before reporting a verified result to the employer.
Employer reporting — only a verified MRO-reviewed result is reported. The employer never sees the raw lab data or the donor’s medical history.
Why the chain matters: Skipping any step — especially MRO review — exposes the employer to wrongful-termination, ADA, and state-law liability. The point of the protocol is not just accuracy; it’s defensibility.
How to Read 4-Panel Drug Test Results Correctly
This section is the most important in the article — and the section where the original version of this guide had the rule reversed. The correction below reflects how POC immunoassay strips actually work.
The single rule
Every immunoassay-based rapid drug test follows the same competitive-binding principle:
Result
Control Line (C)
Test Line (T)
Meaning
Negative
Visible
Visible (any intensity, even faint)
Drug not detected at or above the cutoff. No further action.
Non-Negative (presumptive positive)
Visible
No line in T region
Drug detected at or above the cutoff. Send to lab for confirmation.
Invalid
No C line
Any
Test failed. Discard and repeat with a new device.
The counterintuitive part:A line means negative. No line means non-negative. This is because the test uses competitive binding — when the drug is absent, a labeled drug conjugate freely binds to the test line and produces color. When the drug is present at or above the cutoff, it occupies those binding sites and prevents the conjugate from binding, so no line forms.
What about faint lines?
A faint line in the T region is still NEGATIVE, no matter how faint, as long as it’s visible. Faint lines do not indicate “trace amounts” or “borderline use” — line darkness reflects test mechanics (cutoff levels, reagent age, hydration), not drug concentration. SAMHSA-aligned operating procedures explicitly forbid terms like “faint negative,” “trace,” or “inconclusive” in documentation. Use only Negative, Non-Negative (presumptive positive), or Invalid.
Why this matters for employers
A non-negative POC result is not a positive drug test — and treating it as one is one of the fastest paths to a wrongful-termination claim. Approximately 0.1–0.3% of federal workplace urine specimens confirm positive for fentanyl after laboratory testing, and similar drop-off rates apply across substances when comparing screen-positives to lab-confirmed-positives. The screen exists to identify which specimens warrant the more expensive lab confirmation — not to decide employment.
Panel vs. 5-Panel vs. DOT vs. SAMHSA: What’s the Difference?
Test Type
Substances Covered
Regulated By
Use Case
4-Panel (No-THC)
Amphetamines, cocaine, opiates, PCP
Employer-defined; not federally standardized
Non-DOT workplaces in states with legalized recreational cannabis
Healthcare, public safety, treatment compliance, high-risk industries
Hair follicle test
Same drug classes; longer detection window (up to 90 days)
Not federally regulated for DOT
Pre-employment for high-security or executive roles
Oral fluid (saliva)
Drug classes per panel selected
DOT-authorized since 2023; SAMHSA OFMG effective Oct 2023
Increasingly used for post-incident and reasonable-suspicion testing (harder to adulterate; collection is observed by default)
Critical distinctions for compliance leaders
DOT-regulated employees cannot be tested with a 4-panel for their DOT compliance testing. They must receive the federally mandated 5-panel under 49 CFR Part 40 — even if your company also uses 4-panel for non-DOT staff.
State law preempts portions of employer testing rights in many states. Cannabis-legalization states (NY, NJ, CA, WA, NV, IL, and others) restrict THC testing for non-safety-sensitive positions.
The SAMHSA federal panel and the DOT panel are not identical — DOT harmonizes on a delayed cycle. For example, fentanyl was added to SAMHSA panels in 2025 but DOT harmonization is still pending as of the most recent NPRM (September 2025).
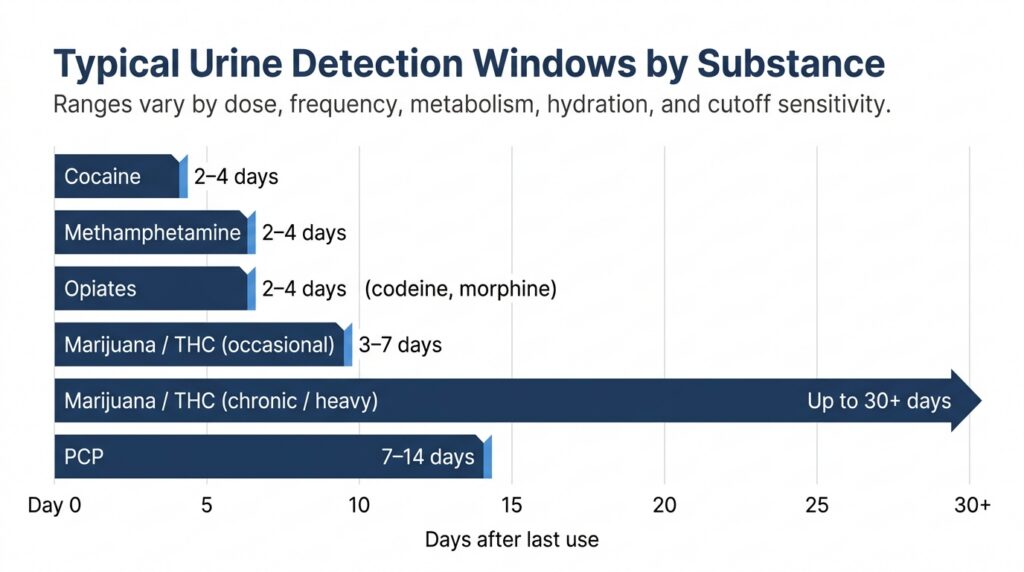
Detection Windows by Substance
Detection windows depend on dose, frequency of use, individual metabolism, age, body composition, hydration, and the cutoff sensitivity of the test. Typical urine detection windows for occasional use:
Substance
Typical Urine Detection Window
Cocaine
2–4 days
Methamphetamine / amphetamines
2–4 days
Opiates (codeine, morphine, heroin metabolites)
2–4 days
Marijuana / THC — occasional use
3–7 days
Marijuana / THC — chronic / heavy use
Up to 30 days or longer
PCP
7–14 days
Benzodiazepines (not in 4-panel)
3–14 days (longer-acting types longer)
Fentanyl (not in standard 4-panel)
1–3 days
Important: These are typical ranges from peer-reviewed literature, not guarantees. Detection windows vary widely between individuals. Cutoff levels also matter: a more sensitive cutoff extends the detection window.
Cutoff Levels and Why They Matter
A cutoff level is the concentration threshold at which a test reports a positive result. Cutoffs are set to balance sensitivity (catching real positives), specificity (avoiding false positives from passive exposure or trace metabolites), and consistency across laboratories.
The SAMHSA Mandatory Guidelines establish standard cutoffs for federal workplace testing — and most non-federal labs adopt the same cutoffs voluntarily for defensibility:
Substance
Initial Test Cutoff (Screening)
Confirmatory Test Cutoff (GC-MS/LC-MS/MS)
Marijuana metabolites (THCA)
50 ng/mL
15 ng/mL
Cocaine metabolites (BE)
150 ng/mL
100 ng/mL
Opiates (morphine, codeine)
2,000 ng/mL
2,000 ng/mL
6-Acetylmorphine (heroin metabolite)
10 ng/mL
10 ng/mL
Amphetamines (incl. meth)
500 ng/mL
250 ng/mL
PCP
25 ng/mL
25 ng/mL
Fentanyl (federal panels, effective July 2025)
1 ng/mL
1 ng/mL
Norfentanyl (urine confirmatory)
n/a
1 ng/mL
Why employers should care about cutoffs: Lower cutoffs catch more positives but also more legitimate medication use that the MRO has to clear. Higher cutoffs reduce MRO workload but may miss low-level use. Most non-regulated employers default to SAMHSA cutoffs because they’re defensible in court and consistent across vendors.
When Employers Use 4-Panel Drug Tests
Standard testing scenarios for non-DOT workplaces:
Pre-employment screening — most common use; often a condition of a job offer.
Random testing — periodic, unannounced, statistically random selection of employees in safety-sensitive or high-risk roles.
Post-incident / post-accident testing — following workplace injuries, near-misses, equipment damage, or other incidents where impairment could be a factor.
Reasonable suspicion testing — based on documented, contemporaneous, articulable observations of behavior, appearance, speech, or odor.
Return-to-duty testing — after a documented violation and completion of an evaluation by a Substance Abuse Professional (SAP).
Follow-up testing — periodic unannounced testing for a defined period (often 1–5 years) following a return-to-duty.
Each scenario carries its own legal documentation requirements. Reasonable-suspicion testing especially requires trained supervisors and contemporaneous written documentation — without it, the test result may be inadmissible.
Legal & Compliance Considerations
Workplace drug testing operates at the intersection of federal, state, and local law. A defensible program addresses all three:
Drug-Free Workplace Act of 1988 — applies to federal contractors and grantees; requires a written policy and employee notification, but does not itself mandate testing.
DOT 49 CFR Part 40 — mandatory testing protocols for safety-sensitive transportation employees.
HHS / SAMHSA Mandatory Guidelines — federal workplace testing under EO 12564.
State law — varies enormously. Recreational cannabis states often restrict pre-employment THC testing for non-safety-sensitive roles. Some states require advance notice, MRO review, or limit testing to specific scenarios.
Americans with Disabilities Act (ADA) — protects individuals in recovery from substance use disorder; current illegal drug use is not protected.
Family and Medical Leave Act (FMLA) — interacts with substance abuse treatment leave.
Title VII of the Civil Rights Act — drug-testing programs cannot be applied in discriminatory patterns.
Local ordinances — some cities (NYC and others) have restricted pre-employment THC testing for most positions.
A drug-testing program that doesn’t account for the state(s) where employees actually work — not just the state where the employer is headquartered — is the single most common source of legal exposure.
Frequently Asked Questions
What does a 4-panel drug test look for?
A 4-panel drug test screens for four drug classes — most commonly the “no-THC” configuration (amphetamines, cocaine, opiates, PCP) used by employers in states with legalized recreational cannabis, or the classic configuration (THC, cocaine, opiates, amphetamines). Unlike the federal 5-panel, the 4-panel composition is set by the employer or testing provider rather than a national standard.
How do you read a 4-panel drug test correctly?
A visible line in the Test (T) region — even a faint one — means negative for that substance, as long as a Control (C) line is also visible. No line in the T region (with a C line present) means non-negative / presumptive positive and requires lab confirmation. No C line means the test is invalid and must be repeated. Line darkness in the T region does not indicate drug concentration — it reflects test mechanics.
Does a faint line mean a positive result?
No. Any visible line in the T region is negative, regardless of how faint. Faint lines reflect cutoff levels and competitive-binding mechanics, not drug concentration. Documentation should never use the term “faint positive” — only Negative, Non-Negative (presumptive positive), or Invalid.
Is a 4-panel test the same as a DOT drug test?
No. DOT-regulated safety-sensitive employees (truck drivers, pilots, transit, rail, pipeline, maritime workers) must be tested with the 5-panel under 49 CFR Part 40, which screens for marijuana, cocaine, amphetamines (including methamphetamine and MDMA), opioids (including semi-synthetic prescription opioids and the heroin metabolite 6-AM), and PCP. A 4-panel cannot satisfy DOT compliance.
Does a 4-panel drug test detect fentanyl?
No, not by default. Standard opiate immunoassays do not detect fentanyl or other synthetic opioids. Fentanyl detection requires either an explicit add-on panel or an expanded panel (9-, 10-, or 12-panel). Note that fentanyl was added to the SAMHSA federal workplace panel effective July 7, 2025, and DOT is in the process of harmonizing — but this is not automatic for non-regulated 4-panel tests.
Does a 4-panel drug test detect benzodiazepines (Xanax, Valium, Ativan)?
No. Benzodiazepines are not part of the standard 4-panel and require an explicit add-on or an expanded panel.
How long does a substance stay detectable in urine?
Typical ranges for occasional use: cocaine 2–4 days, methamphetamine 2–4 days, opiates 2–4 days, THC 3–7 days for occasional users (up to 30+ days for chronic heavy users), PCP 7–14 days. Detection windows vary widely based on dose, frequency, metabolism, hydration, and cutoff sensitivity.
Can I get a false positive or false negative on a 4-panel drug test?
Both are possible but uncommon when the test is administered correctly. False positives can be caused by certain over-the-counter and prescription medications, food products, or laboratory error — which is why every non-negative POC result must be confirmed by a SAMHSA-certified laboratory using GC-MS or LC-MS/MS, then reviewed by a Medical Review Officer (MRO) before any employment action.
How reliable is a 4-panel drug test?
POC immunoassay screens are highly reliable for their intended purpose: distinguishing specimens that need lab confirmation from those that don’t. They are not, by themselves, sufficient evidence to support an employment decision. A complete defensible chain — POC screen → lab confirmation → MRO review → verified result — is what makes a drug-testing program reliable in practice and defensible in court.
How much urine is needed for a 4-panel drug test?
Federal protocols require at least 45 mL for a primary specimen and split specimen. Many non-regulated 4-panel collections accept 30 mL as a minimum. Below 30 mL, the test is generally invalid and the donor is given an opportunity to provide a sufficient specimen.
How long does a 4-panel drug test take?
Initial collection and screening take roughly 15–30 minutes at the collection site. POC results read within about 5 minutes of strip exposure. Negative results are typically reported same-day. Non-negative results reported as verified positive by the MRO usually take 2–4 business days, depending on lab workflow and donor availability for MRO interview.
What’s the difference between a 4-panel drug test and a 4-panel drug screen?
In informal usage they’re interchangeable, but technically a “screen” is the initial immunoassay and a “test” can refer to the full process including lab confirmation. For consistency, treat the POC step as a screen and the laboratory-confirmed, MRO-reviewed result as the test.
How Acuity International Supports Workplace Drug Testing
Acuity International designs and operates drug and alcohol testing programs for non-DOT workplaces, DOT-regulated fleets, federal contractors, and safety-sensitive industries — backed by a network of more than 11,000 credentialed providers across the U.S. and its territories.
Our drug testing services include:
Custom POC and lab-based drug panels — 4-, 5-, 9-, 10-, and 12-panel configurations, plus oral fluid and hair testing where appropriate.
DOT-compliant drug and alcohol testing under 49 CFR Part 40 — including pre-employment, random, post-incident, reasonable suspicion, return-to-duty, and follow-up testing.
SAMHSA-certified laboratory partnerships with full chain-of-custody documentation.
In-house Medical Review Officer (MRO) services — over 1,500 MRO services performed annually, covering both regulated (DOT) and non-regulated testing.
Onsite, mobile, and clinic-based collection options to fit dispersed and remote workforces.
Centralized, secure reporting with real-time program tracking.
Acuity’s drug testing program integrates with our broader occupational health services — physicals, fit-for-duty exams, medical surveillance, and behavioral health — so employers get a single, coordinated workforce-health partner.
This website stores cookies on your computer. These cookies are used to improve your website experience and provide more personalized services to you, both on this website and through other media. To find out more about the cookies we use, see our Privacy Policy.
We won't track your information when you visit our site. But in order to comply with your preferences, we'll have to use just one tiny cookie so that you're not asked to make this choice again.
Choose how we use your data
Through our own and third-party tracking technologies like cookies, pixels, and web beacons, we collect and share with third parties Internet or other electronic network activity and personal identifiers, including IP addresses and device identifiers, to allow the website to function, store your preferences, analyze your website usage, personalize your experience, analyze the performance of our advertising campaigns, and offer you advertisements that target your particular interests.
Our use of third-party cookies may be considered a sale or sharing, including targeted advertising, under state data privacy laws. You can accept all cookies, reject all non-essential cookies, or manage your preferences by category. If we detect an opt-out preference signal such as Global Privacy Control, we will honor it. For additional information and retention terms for trackers, please see our Privacy Notice.
▸ Necessary CookiesAlways Active
These cookies are necessary for the website to function and cannot be switched off in our systems. They are usually set in response to actions you take, such as setting privacy preferences or filling in forms.
▸ Analytics Cookies
These cookies allow us to count visits and traffic sources so we can measure and improve the performance of our site (e.g. Google Analytics).
▸ Advertising Cookies
These cookies may be set through our site by our advertising partners to build a profile of your interests and show you relevant ads on other sites.
▸ Functionality Cookies
These cookies enable the website to provide enhanced functionality and personalization, such as remembering your choices and protecting our forms from spam (Google reCAPTCHA).